Discussion
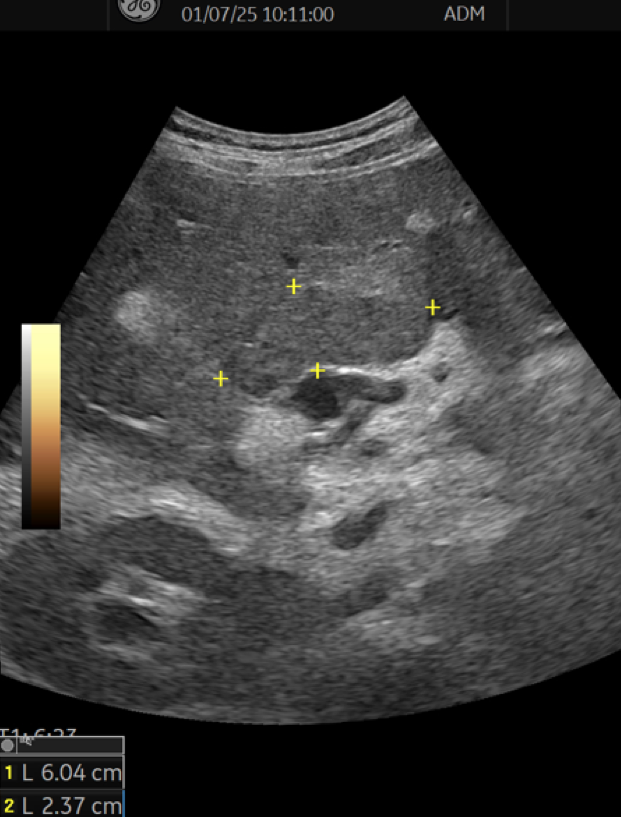
The correct answer is: b) Pedunculated subserosal leiomyoma (FIGO type 7).
Uterine fibroids are the most common benign tumors of the female genital tract, with high lifetime prevalence.¹
Ultrasound is the first-line imaging modality, allowing morphological characterization according to the MUSA consensus, including echogenicity, acoustic shadowing, and vascular patterns.²
Pedunculated subserosal leiomyomas (FIGO type 7) are less common and may represent a significant diagnostic pitfall, as they can mimic solid adnexal masses. In these cases, the pedicle may not be visualized, particularly when it is long and thin.³
The most reliable feature for differential diagnosis is the clear identification of both normal ovaries, separate from the lesion, which effectively excludes adnexal origin. Dynamic assessment may demonstrate synchronous mobility with the uterus, supporting a uterine origin; however, this finding may be limited in cases with long pedicles.
Conclusion
Identification of normal ovaries is the most reliable criterion to differentiate a pedunculated leiomyoma from a solid ovarian tumor. Dynamic ultrasound assessment may be helpful but has limitations in cases with long pedicles.
What are the possible complications of this condition?
Reported complications include:
- Pedicle torsion, a rare event that may present with acute abdominal pain and hemoperitoneum
- Parasitic leiomyoma, resulting from complete loss of uterine attachment
References (Vancouver)
- Stewart EA, Laughlin-Tommaso SK. Uterine fibroids. N Engl J Med. 2024;391:1721–1733.
- Van den Bosch T, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the MUSA group. Ultrasound Obstet Gynecol. 2015;46(3):284–298.
- Oukassem S, Abourak C, Guennouni A, et al. A large pedunculated subserosal myoma with cystic and red degeneration: a case report and literature review. Radiol Case Rep. 2019;14(1):77–82.
- Tsai YJ, Yeat SK, Jeng CJ, et al. Torsion of a uterine leiomyoma. Taiwan J Obstet Gynecol. 2006;45(4):333–335.
- Levai AM, Roar IC, Muresan D. Torsion of a uterine leiomyoma—a rare cause of hemoperitoneum: case report and review of the literature. Med Ultrason. 2019;21(1):77–82. doi:10.11152/mu-1784.
Discussion
The correct answer is: b) Pedunculated subserosal leiomyoma (FIGO type 7).
Uterine fibroids are the most common benign tumors of the female genital tract, with high lifetime prevalence.¹
Ultrasound is the first-line imaging modality, allowing morphological characterization according to the MUSA consensus, including echogenicity, acoustic shadowing, and vascular patterns.²
Pedunculated subserosal leiomyomas (FIGO type 7) are less common and may represent a significant diagnostic pitfall, as they can mimic solid adnexal masses. In these cases, the pedicle may not be visualized, particularly when it is long and thin.³
The most reliable feature for differential diagnosis is the clear identification of both normal ovaries, separate from the lesion, which effectively excludes adnexal origin. Dynamic assessment may demonstrate synchronous mobility with the uterus, supporting a uterine origin; however, this finding may be limited in cases with long pedicles.
Conclusion
Identification of normal ovaries is the most reliable criterion to differentiate a pedunculated leiomyoma from a solid ovarian tumor. Dynamic ultrasound assessment may be helpful but has limitations in cases with long pedicles.
What are the possible complications of this condition?
Reported complications include:
- Pedicle torsion, a rare event that may present with acute abdominal pain and hemoperitoneum
- Parasitic leiomyoma, resulting from complete loss of uterine attachment
References (Vancouver)
- Stewart EA, Laughlin-Tommaso SK. Uterine fibroids. N Engl J Med. 2024;391:1721–1733.
- Van den Bosch T, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the MUSA group. Ultrasound Obstet Gynecol. 2015;46(3):284–298.
- Oukassem S, Abourak C, Guennouni A, et al. A large pedunculated subserosal myoma with cystic and red degeneration: a case report and literature review. Radiol Case Rep. 2019;14(1):77–82.
- Tsai YJ, Yeat SK, Jeng CJ, et al. Torsion of a uterine leiomyoma. Taiwan J Obstet Gynecol. 2006;45(4):333–335.
- Levai AM, Roar IC, Muresan D. Torsion of a uterine leiomyoma—a rare cause of hemoperitoneum: case report and review of the literature. Med Ultrason. 2019;21(1):77–82. doi:10.11152/mu-1784.











{kind=link}